

Asthma is a hypersensitivity reaction to a trigger like exercise, allergies, viruses, smoke, etc. Regardless of trigger, the body initiates an allergic response with a release of inflammatory products that result in a constricted airway, mucus production and airway restriction. I compare it to my sister and I in the woods. She stumbles into some poison ivy and develops an unfortunate itchy rash (normal reaction). I stumble into some poison ivy and my eyes swell shut and everything gets squishy and itchy (exaggerated response). Same exposure, but different reactions. Asthma is this topical reaction, but in the lungs. Symptoms include cough, shortness of breath, fatigue, and weakness.
Asthma is typically a clinical diagnosis meaning there is not a simple test that can be run to confirm so getting a good history is essential. X-rays and blood tests can be helpful, but the history is what makes the diagnosis. Pulmonary function tests and spirometry are the most reliable test to aid in diagnosis, but they can also be normal when asthma not flared. They can also take a while to schedule this test as it should only be administered by a qualified respiratory therapist. The tests consist of measuring airflow speed and volumes. Identifying the triggers can be even more difficult.
The purpose of this post is to talk about the basic medications used for asthma. I don’t know everything about taking care of patients, but I have picked up a few things. If patients don’t feel comfortable with what they are putting in their bodies, they won’t do it. If patients don’t feel like their medications are helping them, they won’t do it. I’m deliberately keeping the explanations simple. I can complicate it with doctor speak, but when I’m talking to my sick patients in the office, I find simple and direct is best. So let’s get into it.
First step of therapy is always albuterol (the “rescue” inhaler.) This inhalant works directly on receptors in the airway to ease the restriction of tight airways by relaxing the muscles in the airways. Relief can last anywhere from four to six hours, but it will do nothing to ease the underlying inflammation. When the albuterol wears off, the tight airways tend to recur. Because it acts as a stimulant of receptors in other parts of the body, it can cause increased heart rate, tremor, sweating, and excitement/anxiety. This medication is typically administered as an inhaler, but it can also be used in a nebulizer as a mist for smaller children/infants or adults with severe constriction. When used frequently for a prolonged period of time, the receptors become less responsive and the medication loses its benefit.
Steroids are a cornerstone of asthma treatment by reducing the inflammation. They also keep receptors fresh so that albuterol remains effective. The preferred route is always inhaled (ICS – inhaled corticosteroids). By going directly into the lung tissue, it works as a topical and avoids systemic steroid side effects. I liken this effect to wearing a long-sleeved shirt when I’m out in the poison ivy. Even though I am exposed to the allergen, my immune system is kept from reacting to it. Side effects of inhaled steroids are thrush (yeast infection of the mouth), hoarseness and sinus infections. Special consideration for children: there can be a dose-related decrease in height velocity (~1 cm loss in height) even with inhaled steroids. Inhaled steroids are more effective for prevention than for acute exacerbations.
Oral steroids have to travel throughout the entire body before treating the inflammation in the lungs and are reserved only for acute exacerbations. They are never a long-term solution due to toxicities of systemic steroid use. The detrimental side effects of steroids are vast. Dr. Google can answer that question just fine.
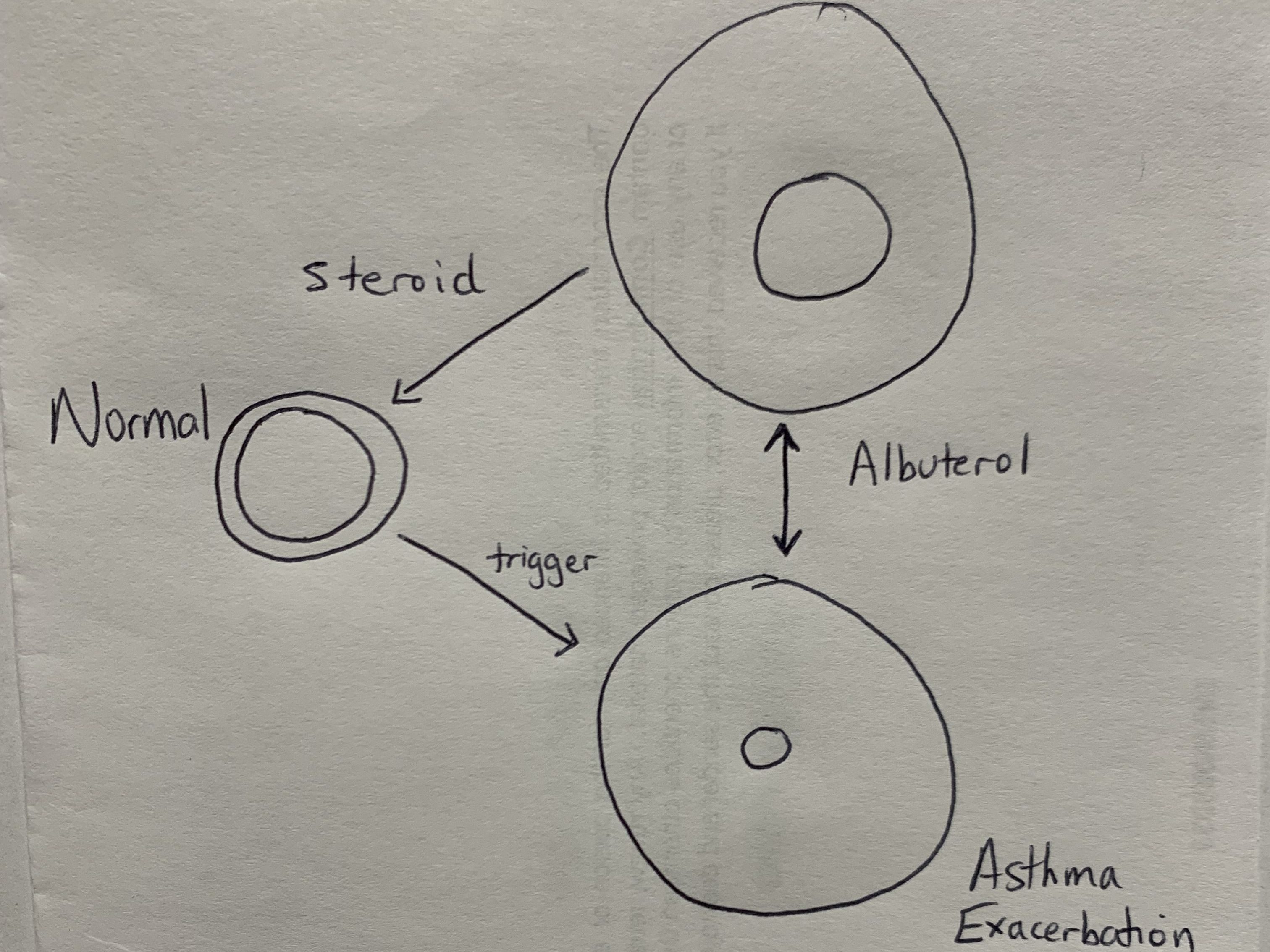
As a visual learner, I drew a simple model to illustrate the difference what happens in the airway after a trigger as well as the effects of albuterol and steroids. Imagine this as a cross-section of your airway with the central areas being your airway and the outer circle being the supporting airway structures. The albuterol works for a while, but unless inflammation addressed, symptoms will typically recur.
Long-acting beta agonists (LABA) are similar to albuterol but have a longer duration of action. They help relax the muscle in the airways but last a lot longer. These meds are not helpful during an acute flare and are utilized for prevention. They have the same side effect profile of albuterol. These are always given with an inhaled steroids for optimal benefit.
Leukotriene Receptor Antagonist work at a cellular level to control inflammation. These are used for prevention and not for acute exacerbations. These meds are less effective than the inhaler therapies, but they have a role when steroids cannot be used. The most concerning side effect of this medication is behavioral problems that may affect a small set of patients.
Criteria used for monitoring disease activity includes frequency of daytime symptoms per week, frequency of nocturnal awakenings per month, frequency of using albuterol for symptom relief, interference with activities between exacerbations, frequency of using oral steroids per year, and abnormalities of pulmonary function testing. The clinician will use this information to determine disease activity and severity.
In deciding which medications to use, medical professionals follow a step program established by specialists. We use the patient’s symptoms and response to therapy to classify their disease based on frequency and severity of symptoms the follow that protocol. The medications can then be adjusted to achieve the desired effect of normal activity tolerance.
A combination of the previously mentioned meds is used to control the majority of people with asthma. If the above meds are not adequate for controlling asthma symptoms, it is time to get a specialist involved.

Leave a comment